Introduction
According to CDC data, an estimated 687,000 hospital-acquired infections (HAIs) occurred in U.S. acute-care facilities in 2015, with roughly 72,000 patients dying during those hospitalizations. On any given day, about 1 in 31 hospitalized patients carries an active HAI.
The financial weight is equally severe. AHRQ estimates average attributable costs at approximately $31,000 per HAI case — with ventilator-associated pneumonia and central line infections approaching $48,000 each.
Airborne pathogens account for a measurable share of that burden. Mycobacterium tuberculosis, Aspergillus spores, measles, and SARS-CoV-2 aerosols all exploit gaps in air quality controls — and those gaps are often an infrastructure problem. HEPA filtration is an active safety system with specific installation, configuration, and maintenance requirements. Gaps in any of those areas translate directly into preventable infections.
This guide covers how HEPA filtration works, zone-specific requirements, safe installation, ongoing monitoring, and the mistakes that create compliance gaps.
Key Takeaways
- True HEPA filters capture ≥99.97% of particles at 0.3 microns; H13 and H14 variants offer higher efficiency for the most critical zones
- ASHRAE Standard 170, CDC guidelines, and The Joint Commission define minimum filter requirements by room type — non-compliance creates both patient safety and regulatory risk
- AIIRs require ≥12 ACH, negative pressure, and HEPA on exhaust; protective environment rooms require HEPA on supply air under positive pressure
- HEPA systems need staged pre-filtration, post-installation leak testing, and condition-based replacement, not visual inspection alone
- Mobile cleaning robots with H13 HEPA filtration add a supplemental floor-level capture layer during cleaning operations, complementing fixed HVAC systems
How HEPA Filtration Controls Airborne Pathogens in Hospitals
The Physics of HEPA Capture
The EPA defines HEPA as a filter that removes at least 99.97% of airborne particles at 0.3 microns — the "most penetrating particle size" (MPPS), meaning it is the hardest size to capture. Three mechanisms make this possible:
- Interception — particles following airflow streamlines contact filter fibers and adhere
- Inertial impaction — heavier particles deviate from airflow and collide with fibers
- Diffusion — the smallest particles (<0.1 µm) move erratically and contact fibers through Brownian motion
Particles both larger and smaller than 0.3 µm are captured more efficiently — which is why MPPS defines the minimum rating standard.
Hospital Pathogens and Why 0.3 µm Matters
The pathogens hospitals must contain fall squarely within HEPA's design range:
| Pathogen | Particle Size | Airborne Risk |
|---|---|---|
| M. tuberculosis | 1–5 µm droplet nuclei | Remains suspended for hours |
| Aspergillus spores | ~2.5–3.0 µm | Critical risk to immunocompromised patients |
| Measles | ~0.5–6 µm aerosol droplets | Infectious in shared air for up to 2 hours |
| SARS-CoV-2 | Primarily <5 µm fine aerosols | Suspended for minutes to hours |
| Pseudomonas aeruginosa | ~1–5 µm aerosol droplets | Cough-generated, gram-negative |
Research supports HEPA's effectiveness against these threats. A 2006 PubMed-indexed study found that portable HEPA filtration reduced MRSA environmental contamination in patient isolation rooms. A 2002 study concluded HEPA filters were protective for immunocompromised hematologic malignancy patients during an Aspergillus outbreak.
HEPA Grade Selection
Not all HEPA filters carry the same efficiency. Mismatching filter grade to zone type isn't a spec footnote — it's a compliance gap with direct patient safety consequences:
- True HEPA (U.S. standard) — ≥99.97% at 0.3 µm; baseline for most clinical areas
- H13 (EN1822) — ≥99.95% at MPPS; appropriate for AIIRs, ORs, and sensitive clinical spaces
- H14 (EN1822) — ≥99.995% at MPPS; highest-risk zones such as stem cell transplant units or BSL-level labs
Selecting the right grade only matters if the surrounding system is also correctly specified. HEPA operates within a multi-barrier strategy — pressure differentials, air change rates, antimicrobial surfaces, and PPE each depend on the others functioning correctly.
A properly specified HEPA filter in a room with inadequate ACH still leaves patients exposed.
HEPA Filter Requirements by Hospital Zone
ASHRAE Standard 170 Framework
ASHRAE Standard 170 governs minimum filter efficiencies in healthcare ventilation systems through a two-bank configuration. Filter Bank 1 provides coarse pre-filtration; Filter Bank 2 handles fine or HEPA-grade filtration for critical spaces. ASHE confirms that MERV 14 or HEPA may be required depending on the space classification.
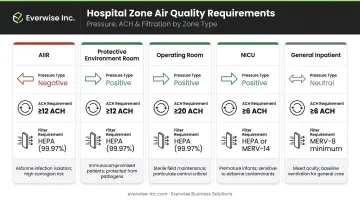
The key zone requirements:
| Zone | Pressure | ACH | Filter Requirement |
|---|---|---|---|
| Airborne Infection Isolation Room | Negative (≥0.01" w.g.) | ≥12 | HEPA on exhaust or direct outdoor exhaust |
| Protective Environment Room | Positive (≥0.01" w.g.) | ≥12 | HEPA on supply air |
| Operating Room | Positive | Per 170 table | MERV 14 minimum; HEPA for high-risk |
| NICU | Positive | Per 170 table | HEPA-filtered supply |
| General Inpatient | Per zone | Per 170 table | MERV 14 typical |
AIIRs vs. Protective Environment Rooms
These two room types are frequently confused. Mixing up their configurations is a direct patient safety hazard.
Airborne Infection Isolation Rooms (AIIRs) contain infectious patients. Key requirements:
- Negative pressure (minimum −2.5 Pa / 0.01″ w.g.) keeps contaminated air from escaping into corridors
- All exhaust must exit directly outdoors or pass through HEPA before recirculation
- At 12 ACH, an empty room achieves 99% contaminant removal in approximately 23 minutes
Protective Environment (PE) Rooms protect immunocompromised patients from incoming pathogens. Key requirements:
- Positive pressure with HEPA on the supply air — not the exhaust
- Every cubic foot of incoming air must be filtered before reaching a patient with no immune defense
- Exhaust air does not require HEPA treatment in this configuration
Reversing these configurations — positive pressure in an AIIR or unfiltered supply in a PE room — creates the exact hazard the room is designed to prevent.
Operating Rooms and NICUs
In ORs, HEPA diffusers are positioned to create laminar or unidirectional airflow directly over the sterile field. This configuration sweeps potential contaminants away from the surgical site rather than allowing recirculation. MERV 14 is the minimum for general OR use; HEPA is recommended for high-risk procedures.
NICUs require HEPA-filtered supply air due to the extreme vulnerability of neonates. Across critical zones — including pharmacy compounding areas and BSL-2 lab spaces adjacent to clinical units — Biological Safety Cabinets must be tested and certified at least annually per NSF/ANSI Standard 49 using aerosol challenge methods. Operational integrity must be re-verified after any repair or relocation.
Safe Installation and System Configuration
Pre-Filtration Staging
HEPA filters must be preceded by pre-filters — typically MERV 11–16 bag or V-bank configurations. Without pre-filtration:
- HEPA media loads prematurely with coarse dust
- Airflow resistance rises faster than expected
- ACH rates drop below required minimums before the filter is "due" for replacement
- Replacement costs increase significantly
Pre-filters capture particles above 1 micron, preserving HEPA media capacity for the sub-micron pathogens that bypass coarser filtration entirely.
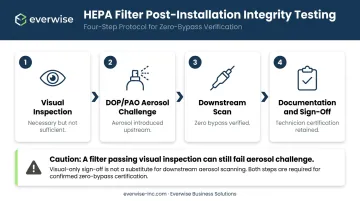
Post-Installation Leak and Integrity Testing
Visual inspection after HEPA installation is not sufficient. Even a hairline gap around a filter frame or gasket allows unfiltered air to bypass the media entirely. Post-installation integrity testing uses a DOP (dioctyl phthalate) or PAO (poly-alpha-olefin) aerosol challenge to verify zero bypass. IEST-RP-CC034 covers procedures for leak-testing HEPA and ULPA filters after installation in cleanrooms and clinical air devices.
A filter that passes visual inspection but fails aerosol challenge testing provides no protection. Test results must be documented and retained as part of the commissioning record — not completed until a qualified technician signs off on a passing scan.
Pressure Verification and Commissioning
After installation, room pressure relationships must be verified with a calibrated manometer or magnehelic gauge. Isolation rooms cannot be cleared for patient use until the correct pressure differential is confirmed and documented.
Commissioning requires both infection control professionals and HVAC technicians present — not one or the other. Installation must stop if any of the following conditions exist:
- Unsealed duct penetrations
- Damaged filter media or frames
- Incorrect filter grade for the assigned zone
- Missing or non-functional pressure monitoring
- Lack of qualified commissioning personnel
Safe Operation, Monitoring, and Common Mistakes
What to Monitor in Operational HEPA Systems
Facility teams should track these indicators continuously:
- Rising differential pressure across the filter bank — the primary replacement trigger per ASHE guidance
- Reduced supply air volume at diffusers, indicating increased media resistance
- Increasing particulate counts on environmental monitoring
- Visible moisture or contamination on filter faces — CDC recommends replacing water-damaged HEPA filters with metal-framed units
Condition-based replacement driven by differential pressure and manufacturer service limits is the established standard. No fixed interval applies across all clinical environments — high-particulate areas load filters faster than low-activity zones.
Safe Filter Change-Out Protocols
HEPA filters in isolation and protective environment rooms must never be changed without containment controls in place. Captured pathogens concentrate on the filter media — disturbing it without precautions re-aerosolizes what the filter spent weeks collecting.
Key requirements before any filter change-out:
- Establish containment barriers before removing filter assemblies
- Use appropriate PPE (N95 minimum) during media handling
- Bag and seal spent filters immediately — do not transport through patient-care corridors unsealed
- For portable units used in construction zones, clean all internal and external surfaces and re-verify filter performance before returning units to patient-care areas (CDC guidance)
Supplemental HEPA During Cleaning Operations
Fixed HVAC HEPA systems have one structural limitation: they cannot rapidly recapture particles resuspended from floor surfaces during cleaning. Floor disturbance — sweeping, vacuuming, and scrubbing — launches settled particles back into the breathing zone before HVAC airflow can pull them toward return registers.
Mobile HEPA-equipped cleaning robots address this gap directly — capturing particles at the point of disturbance rather than waiting for HVAC return cycles. The Gausium Vacuum 40, distributed in Texas by Everwise Business Solutions, carries an H13 medical-grade HEPA filter rated for fine dust and allergen capture during active cleaning.
Deployed in hospital corridors, lobbies, waiting areas, and cafeterias, it functions as a mobile filtration layer alongside fixed HVAC — not as a replacement for it. Everwise offers scheduled preventive maintenance contracts for healthcare facilities that include H13 HEPA filter replacement at each service visit.

Three Mistakes That Create Compliance Gaps
1. Wrong filter grade for the zone. A MERV 14 filter installed in a protective environment room is not a minor spec deviation — it leaves immunocompromised patients exposed while facility records show a "compliant" installation. This is a procurement and specification accountability issue requiring formal zone-by-zone verification.
2. Delayed filter replacement. An occluded filter increases airflow resistance, forces the HVAC system to work harder, and reduces ACH below required minimums. The infection control failure happens before visible degradation appears. Manufacturer schedules and pressure differential thresholds exist precisely because visual inspection cannot detect progressive loading.
3. Neglecting construction and renovation HEPA protocols. Approximately half of healthcare-associated Aspergillus outbreaks are caused by construction or renovation activities near hospitals. APIC's ICRA matrix and ASHE's ICRA 2.0 tool both require portable HEPA-equipped air filtration units and negative pressure containment within construction zones adjacent to patient care areas. The Joint Commission cites pre-construction risk assessment as a formal requirement covering air quality and infection control. Skipping this step is one of the most consistently cited compliance failures in Joint Commission surveys.
Conclusion
HEPA filtration safety in hospitals depends on five things working together:
- Zone-specific specification — matching filter grade to the infection risk of each area
- Staged system design — pressure differentials and air change rates engineered for the zone
- Verified installation — DOP/PAO challenge testing before any patient occupancy
- Monitored operation — continuous pressure differential and airflow alerts
- Scheduled maintenance — documented filter replacement and integrity re-testing on fixed intervals
A gap in any one of these creates an opening that airborne pathogens will exploit.
Hospital facility managers and infection control teams should treat HEPA systems with the same disciplined oversight they apply to medical equipment — documented maintenance logs, staff training, and integration with the facility's infection control risk assessment program. When a filter goes unchecked or an installation skips leak testing, it's not a compliance gap — it's a direct patient safety risk.
Frequently Asked Questions
What HEPA filters do hospitals use?
Hospitals use true HEPA filters (≥99.97% at 0.3 µm) as the baseline, with H13 or H14 medical-grade variants deployed in highest-risk zones such as protective environment rooms and operating suites. Filter selection follows ASHRAE Standard 170 room classifications and must be verified zone by zone.
Are hospitals required to have HEPA filters?
Not every room requires HEPA, but specific areas — protective environment rooms and airborne infection isolation rooms — are mandated under ASHRAE Standard 170, CDC guidelines, and Joint Commission accreditation standards. Non-compliance creates direct patient safety risks and accreditation exposure.
How often should HEPA filters be changed in hospitals?
Replacement is driven by differential pressure readings and manufacturer service limits, not a fixed universal interval. Visual appearance alone cannot confirm filter saturation — continuous pressure monitoring is the only reliable indicator.
What is the difference between MERV 14 and HEPA in a hospital setting?
MERV 14 filters capture 90–95% of particles in the 0.3–1.0 µm range and are appropriate for general inpatient areas and standard OR configurations. HEPA captures ≥99.97% at 0.3 µm and is required where airborne pathogen elimination is critical. The two are used in staged configurations rather than interchangeably.
What are the ACH requirements for hospital isolation rooms?
CDC and ASHRAE Standard 170 require a minimum of 12 ACH for AIIRs, with exhaust directed outdoors or through HEPA before recirculation. Protective environment rooms share the 12 ACH minimum but operate under positive rather than negative pressure.
Can portable HEPA units supplement fixed HVAC HEPA filtration?
Yes. Portable and mobile HEPA units are used during construction, renovation, and in areas where fixed systems cannot achieve required ACH alone. They also address the particle resuspension gap during cleaning operations.