According to Healthy People 2030, 1 in 31 hospitalized patients has at least one HAI at any given time, with more than 680,000 infections occurring annually across U.S. hospitals. Meanwhile, a 2020 peer-reviewed article found that hospital cleaning staff had been reduced by 25% since the mid-1990s, with over a third of hospitals disbanding in-house EVS teams entirely.
Against this backdrop, autonomous cleaning robots have entered the market — and hospital administrators are now wrestling with a real question: automate, stick with traditional janitorial services, or combine both? The answer depends on your facility, your budget, and what your infection control goals actually require.
Key Takeaways
- Cleaning robots operate 24/7 with consistent protocols — best suited for large corridors, lobbies, and predictable floor areas
- Janitorial services provide human judgment, adaptability, and hands-on capability in complex or biohazard situations
- Robots carry significant upfront costs that vary by model, configuration, and facility scale
- A hybrid model is the most effective approach for most hospitals — robots handle floors, humans handle everything else
- Your best option depends on facility size, staffing pressures, budget structure, and HAI reduction targets
Hospital Cleaning Robots vs. Janitorial Services: Quick Comparison
| Factor | Cleaning Robots | Janitorial Services |
|---|---|---|
| Upfront Cost | High (quote-based per unit) | Low to none |
| Ongoing Cost | Lower labor; maintenance + software fees | Recurring labor; subject to wage inflation |
| Availability | 24/7, no absenteeism | Dependent on shift coverage and staffing |
| Consistency | Identical protocol every run | Varies by individual and shift |
| Flexibility | Limited to pre-mapped, open areas | Adapts to any situation or space |
| Infection Control | Advanced (UV-C, HEPA options) | Depends on training and protocol adherence |
| Implementation | Requires mapping, training, contracts | Straightforward service contract |
Cost Breakdown
Robots: Purchase price is quote-based for commercial-grade hospital units, with total cost of ownership including maintenance contracts, software, consumables, battery replacement, and operator training.
Janitorial Services: BLS data shows hospital-sector janitors earn a median hourly wage of $16.47 nationally, with Texas wages slightly lower at $14.50 median. Loaded costs (wages plus benefits) run substantially higher. The BLS reports hospital-sector total compensation averaging $66.73/hour across all roles. EVS-specific loaded rates vary by facility and require internal calculation.
Infection Control Reality
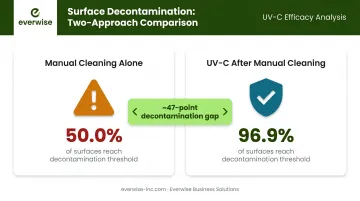
Manual cleaning has a documented consistency problem. A 2021 field study found that more than 50% of surfaces may go untouched during manual cleaning. In the same study, UV-C irradiation after manual cleaning achieved 96.9% surface decontamination, compared to 50.0% for manual cleaning alone.
For facilities managing immunocompromised patients, that nearly 47-point gap in decontamination isn't a minor variable — it's a direct infection control risk.
What Are Hospital Cleaning Robots?
Hospital cleaning robots are autonomous machines that use AI, 3D sensors, and pre-programmed facility maps to navigate and clean healthcare environments independently. Modern units have moved well beyond the basic robotic floor scrubbers of the late 1990s — today's models feature real-time obstacle avoidance, self-docking, and continuous environment adaptation.
Core Functions in Hospital Settings
Three core functions define how these robots are deployed in hospitals:
- Autonomous floor scrubbing and vacuuming — covers large surface areas at consistent intervals without fatigue or human variability
- UV-C surface disinfection — used as an adjunct after manual cleaning to reduce pathogen load on high-risk surfaces
- Air purification with HEPA filtration — captures fine particulates, allergens, and harmful particles during cleaning cycles
Consistent, fatigue-free operation is the core value proposition. A robot running overnight protocols in a hospital corridor doesn't cut corners at 3 a.m. because it's tired or understaffed.
Technology Features That Matter in Hospitals
Not all commercial cleaning robots are built for healthcare demands. Key differentiators include:
- 3D depth cameras with AI floor identification — automatically adjusts cleaning mode and brush height for tile, vinyl, carpet, and other surfaces
- High-precision edge-cleaning sensors — reaches corners and baseboards that standard equipment often misses
- H13 HEPA filtration — meets the medical-grade filtration standard required for clinical air quality, going beyond standard commercial HEPA ratings
These aren't just nice-to-haves — in healthcare settings, each feature addresses a specific infection control or compliance gap. Everwise Business Solutions distributes Gausium's autonomous cleaning robots across Texas, including the Vacuum 40, which is built specifically for healthcare applications. It combines H13 medical-grade air purification, AI-driven floor identification, and zero-distance edge cleaning — all suited for the high-traffic hallways and sensitive environments hospitals operate.

Where Robots Work Best Inside Hospitals
Optimal deployment areas:
- Long corridors and hallways with consistent floor surfaces
- Open waiting areas and lobbies
- Cafeteria floors during off-hours
- Post-discharge room floor prep (prior to terminal cleaning)
- Overnight floor maintenance cycles when traffic is minimal
These predictable, unobstructed spaces allow robots to run complete cleaning cycles with minimal supervision — freeing EVS staff for higher-complexity work.
What Are Janitorial Services in Hospitals?
Hospital janitorial services — more accurately called Environmental Services (EVS) — encompass far more than mopping floors. Contracted or in-house EVS teams handle a range of clinical cleaning tasks, from general common-area maintenance to specialized work that requires training, judgment, and direct coordination with nursing staff.
What Makes Human EVS Staff Irreplaceable
There are capabilities robots simply cannot replicate right now:
- Recognizing unexpected hazards on the spot: broken glass, biohazard spills, patient falls
- Cleaning under furniture and in confined spaces that robots can't physically navigate
- Handling non-cleaning duties like restocking supplies, relaying room status to nursing staff, and fielding urgent requests
- Managing biohazard and regulated medical waste, which requires trained personnel and verified protocol at every step
The U.S. healthcare environmental services market was valued at $6.76 billion in 2024 and is projected to reach $9.53 billion by 2029 — reflecting sustained, growing demand for human EVS work in healthcare. That growth, however, masks a persistent operational challenge.
The Staffing Challenge
The structural problem facing hospital janitorial programs is hard to ignore. The 2020 peer-reviewed analysis noted that 83% of EVS personnel reported having to train new recruits on the job — a signal of chronic turnover pressure and the institutional knowledge lost when experienced staff leave. When experienced staff cycle out frequently, cleaning consistency deteriorates — and that inconsistency has a direct effect on HAI rates.
A separate 10-year hospital study found that when cleaning performance improved from 74.7% to over 90%, HAI rates dropped by 75%. The corollary is equally important: when cleaning performance deteriorates due to understaffing or high turnover, infection rates climb.
Tasks Where Human Staff Remain Essential
- Isolation room terminal cleaning following infectious patients
- Operating room turnovers requiring judgment and protocol verification
- Bathroom and high-touch surface disinfection in patient rooms
- Any situation involving bodily fluids or regulated medical waste
- Audits, compliance documentation, and nursing communication
Current robotic technology has no practical role in any of these tasks.
Which Cleaning Solution Is Right for Your Hospital?
The honest answer for most hospitals: both. But the mix depends on your specific facility.
Key Evaluation Criteria
Before choosing a path, assess these factors:
- Facility size and floor plan complexity — robots need sufficient open square footage to justify the investment
- Current staffing situation — chronic vacancies or high turnover strengthen the case for automation
- Budget structure — can you absorb capital expenditure, or do operating expense contracts fit better?
- HAI rates and infection control goals — facilities with elevated HAI rates may see faster ROI from robot-assisted disinfection
- Regulatory requirements — CMS 42 CFR 482.42 requires hospitals to maintain active infection control programs and sanitary environments; your cleaning strategy must support compliance
Building a ROI Framework
There's no universal payback timeline — anyone claiming one without facility-specific data is guessing. Instead, use this framework:
- Calculate your true labor cost — hourly wage plus benefits, overtime, agency labor during vacancies, and turnover-related training costs
- Map your cleanable square footage — identify open, robot-suitable areas separately from complex patient-care zones
- Get unit-specific quotes — total cost of ownership includes purchase price, maintenance contracts, software, consumables, and battery replacement
- Model coverage hours — how many labor hours per week does the robot replace, and at what loaded cost?
- Set a breakeven threshold — divide total 3-year robot cost by your loaded hourly labor rate to determine how many labor hours must be offset

Frederick Health Hospital's T7AMR deployment offers a real-world reference point: the robot cleaned approximately 20,000 sq ft daily in autonomous mode, with staff redeployed to patient-room disinfection, more frequent bathroom cleaning, and patient interaction — qualitatively positive ROI without publishing a specific payback period.
Situational Recommendations
Choose cleaning robots if your hospital has:
- Large open corridors and floor areas (lobbies, waiting rooms, cafeteria)
- Chronic EVS staffing shortages or high vacancy rates
- High overnight cleaning demands with limited shift coverage
- Aggressive HAI reduction goals requiring consistent floor sanitization
Rely primarily on janitorial services if your facility has:
- Complex layouts with many confined or irregular spaces
- Smaller footprint where robot capital cost is hard to justify
- Primarily patient room-focused cleaning needs
- Budget constraints that make upfront investment impractical
How a Hybrid Model Works in Practice
For most hospitals, the right answer isn't a choice between robots and people — it's designing a program where each handles what it does best.
Robots take on repetitive floor coverage in high-traffic, open areas. EVS staff focus on patient rooms, isolation areas, bathrooms, high-touch surfaces, and exception handling. Assigning trained EVS staff to supervise robot operation instead of clinical cleaning tasks wastes the value of both. A well-designed hybrid avoids that trap.
The practical risk of going all-in on either option:
- Over-reliance on robots creates gaps in complex or unexpected cleaning scenarios
- Over-reliance on janitorial services leaves facilities exposed to labor volatility and inconsistency during understaffed shifts
The most durable programs pair both — robots handling predictable, high-volume floor coverage while staff concentrate on the complex, human-judgment work robots can't replicate.
Conclusion
For large hospitals with staffing challenges and consistent open floor plans, cleaning robots deliver measurable gains in consistency and infection control. For smaller facilities or those with complex layouts and primarily room-based cleaning needs, janitorial services remain the backbone. For most hospitals, a thoughtfully structured hybrid model is the most durable approach, backed by real-world deployments across a range of facility types.
What's at stake in these decisions is concrete: facilities that get this right see lower HAI rates, reduced long-term labor costs, and an EVS program resilient enough to absorb staff turnover without compromising cleanliness standards.
Texas healthcare facilities looking to put that hybrid approach into practice can reach Everwise Business Solutions — the authorized Gausium distributor for Texas — at 210.884.0559 or german.zavala@everwise-inc.com. Their team will match the right models to your facility's floor plan, staffing situation, and infection control priorities.
Frequently Asked Questions
How do hospital cleaning robots compare to janitorial services?
Robots provide consistent, 24/7 floor coverage and disinfection without fatigue or absenteeism — ideal for high-traffic corridors and large open areas. Janitorial services provide the human judgment, flexibility, and biohazard capability that robots currently cannot replicate. Most hospitals benefit from using both in a coordinated program.
How much do hospital cleaning robots typically cost?
Commercial-grade hospital cleaning robots are quote-based, with pricing varying by model, configuration, and vendor. Total cost of ownership includes maintenance contracts, software, consumables, and battery replacement — not just purchase price. Everwise Business Solutions offers Texas-based guidance on financing and leasing arrangements.
What are the main types of service robots used in hospitals?
Healthcare facilities rely on three main categories: autonomous floor scrubbers and vacuums for large surface areas, UV-C disinfection robots used as adjuncts after manual cleaning, and hybrid units combining floor scrubbing with HEPA air filtration. Each addresses a different layer of hospital hygiene.
Can cleaning robots fully replace janitorial staff in hospitals?
No. Current robots cannot handle biohazards, confined spaces, vertical surfaces, patient room complexity, or situations requiring real-time judgment. They are designed to complement trained EVS staff — handling repetitive floor tasks so humans can focus on higher-value clinical cleaning.
What hospital areas are best suited for cleaning robots?
Large, open, predictable spaces work best: corridors, lobbies, waiting rooms, and cafeterias. Patient rooms, bathrooms, isolation units, and operating rooms still require human cleaning staff — these areas involve too many variables, high-touch surfaces, and potential biohazards for current autonomous technology to manage reliably.
What is the ROI timeline for a hospital cleaning robot investment?
ROI depends on your facility's loaded labor costs, cleanable square footage, and cleaning frequency requirements — no universal timeline applies. Some hospitals achieve breakeven within 12–24 months through labor redeployment and improved cleaning efficiency, but this requires facility-specific modeling rather than generic industry estimates.